Anatomy of the Esophagus
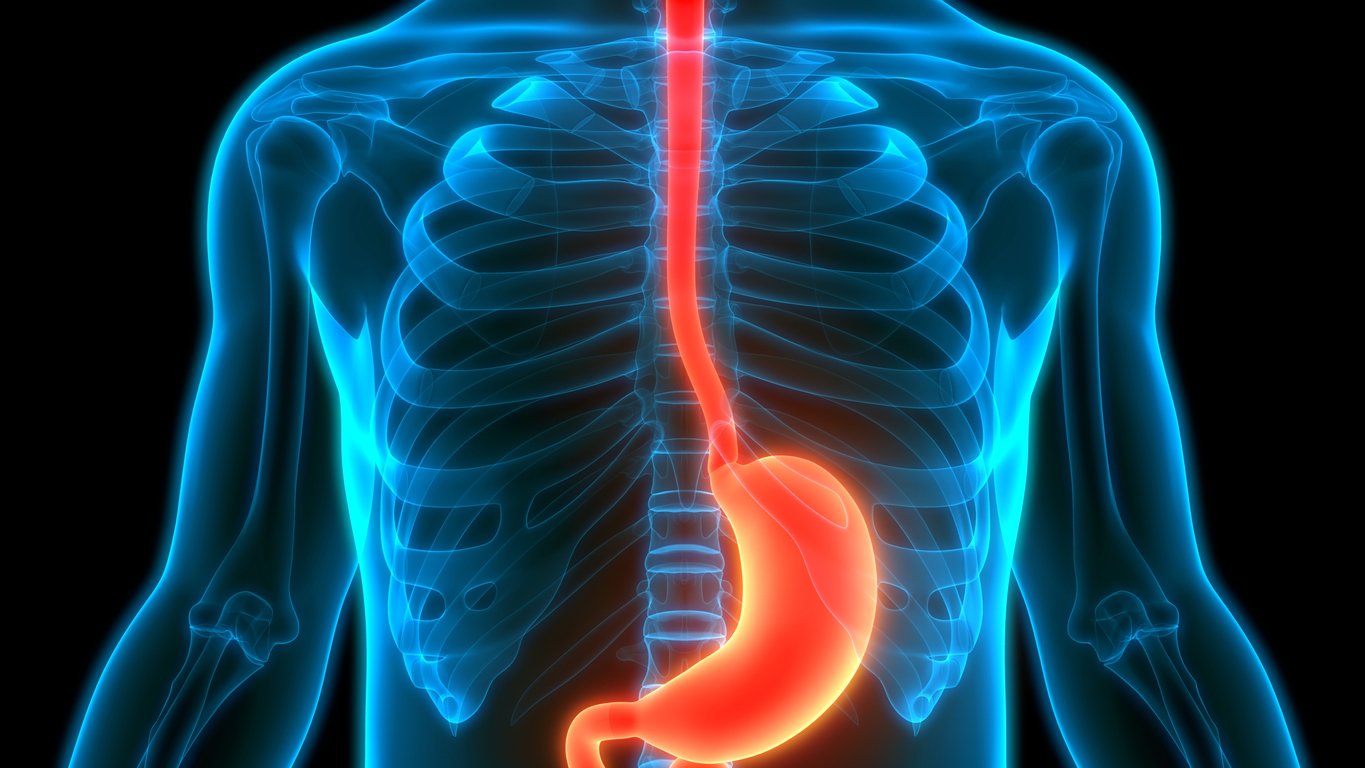
The esophagus is a tubular, hollow organ that transports food from the mouth to the stomach. It is divided into three sections and also has three physiological constrictions. A complex closure mechanism seals the esophagus from the stomach. Histologically
the esophagus is structured in the same way as the other organs of the gastrointestinal tract, with a few exceptions.
Profile of the Esophagus:
Function: Food transport
Location: Begins at the lower border of the cricoid cartilage of the larynx and ends where it joins the stomach
Shape: Tubular
Length: 25–30 cm
Topography:
Topography:
Course
C6-C7: Transition from the pharynx to the esophagus (esophageal mouth = upper esophageal sphincter) runs between the trachea and the spine into the thorax;
Th4: Aorta lies against the esophagus from the left (aortic constriction);
Continues through the posterior mediastinum;
Left: Aorta; Right: Right lung; Ventral: Left atrium; Dorsal: Spine
Th10: Esophagus passes together with the vagal trunks through the esophageal hiatus of the diaphragm (= diaphragmatic constriction);
Continues caudally along the left liver lobe;
Th11: Esophagus, empties into the stomach.
Structure
The esophagus is a muscular tube that is divided into three sections based on its location. Along its course, the esophagus has three constrictions, which are caused by its relationship to adjacent structures. At the lower end of the esophagus, an interplay of various mechanisms ensures the closure of the esophagus to the stomach entrance (= pars cardiaca); there is no true sphincter muscle.
Sections
Cervical part of the esophagus (= cervical portion)
- Length: 7–8 cm
- Course: From the lower border of the cricoid cartilage to the superior thoracic aperture
Thoracic part of the esophagus (= thoracic portion)
- Length: 16 cm
- Course: From the superior thoracic aperture to the diaphragmatic passage
Abdominal part of the esophagus (= abdominal portion)
- Length: 1–3 cm
- Course: From the diaphragmatic passage to the entry into the stomach
- The abdominal part of the esophagus (= pars abdominalis) is intraperitoneal!
- The angle at which the pars abdominalis of the esophagus enters the stomach is called the “angle of His”!
Closure mechanism of the lower esophagus (= Lower Esophageal Sphincter, LES)
- Spirally arranged esophageal muscle layer
- Pressure gradient between thoracic and abdominal cavity
- Acute angle of entry of the esophagus into the stomach (angle of His)
- Venous plexus of the esophagus
- Diaphragmatic constriction
- Fixation of the esophageal end by the phrenicoesophageal ligament (= Laimer’s membrane)
Collectively, these closure mechanisms are referred to as the lower esophageal sphincter (LES). However, it is not a true sphincter but a functional sphincter system!
Diseases of the Esophagus
- Reflux esophagitis and Barrett’s esophagus:
If the mechanism of the lower esophageal sphincter does not function correctly, there is a backflow (= reflux) of gastric juice into the esophagus. The esophageal epithelium provides mechanical but not chemical protection. Since gastric juice consists, among other things, of very aggressive hydrochloric acid, reflux can lead to inflammation of the esophagus (= esophagitis). This condition is called “reflux esophagitis”. Symptoms of reflux esophagitis are retrosternal pain (= heartburn), which occurs mainly after eating and when lying down. If reflux esophagitis persists for a longer period, the normal esophageal epithelium (stratified non-keratinized squamous epithelium) can transform into columnar epithelium (= metaplasia). Such a transformation is referred to as “Barrett’s esophagus”, on the basis of which dysplasias can develop as a precursor to carcinoma. - Esophageal varices:
Between the drainage area of the inferior vena cava and the portal vein, there are collateral circulations (these are called “portocaval anastomoses”). If blood outflow into the portal vein is impeded (e.g., by liver cirrhosis), the blood bypasses the liver and backs up into the collateral circulations. It then flows, for example, via the veins of the esophagus into the superior vena cava. However, since these veins are not designed for such high pressure, they distend. These dilated veins – so-called esophageal varices – can rupture and lead to life-threatening bleeding. - Esophageal diverticula (e.g., Zenker’s diverticulum):
Like the rest of the digestive tract, the esophagus has an inner circular muscle layer and an outer longitudinal muscle layer. This is not equally strong at all points in the esophagus. For example, it is often absent on the dorsal side of the esophagus (lower border of the inferior pharyngeal constrictor muscle, cricopharyngeal part), in the so-called Laimer’s triangle, and at the transition from the pharynx to the esophagus (between the fundiform part and the oblique part of the inferior pharyngeal constrictor muscle), the so-called Killian’s triangle. When pressure in the esophagus increases, at these two locations - mucosal outpouchings (= pulsion diverticula) can occur, where the tunica mucosa and tela submucosa are pushed outwards through the muscle layer. Since not all layers of the wall are affected, these are referred to as “false diverticula” or “pseudodiverticula”. If such a diverticulum occurs in Killian’s triangle, it is called a Zenker’s diverticulum. Although it is treated as an esophageal diverticulum, anatomically it originates from the hypopharynx. “True diverticula”, in which all layers of the wall protrude, arise independently of muscular weak points and are also called “traction diverticula”.
- Esophageal achalasia: Achalasia is a functional disorder of the esophageal musculature and the lower sphincter.
- Esophageal carcinoma: Histologically, a distinction is made between squamous cell carcinomas in areas where the esophagus has squamous epithelium, often caused by noxious agents such as alcohol and nicotine.
In addition, there is adenocarcinoma at the junction of the esophagus and stomach.